Nutrition
Malnutrition is present in approximately 45% of patients at time of admission to hospital. It is often underrecognized and is associated with increased postoperative complications and in-hospital and 30-day mortality. Nutrition risk is also associated with increased length of stay, readmission, and hospital costs. (1-5) Preoperative & early postoperative nutritional intervention are associated with improvements in postoperative complications and mortality. (6)
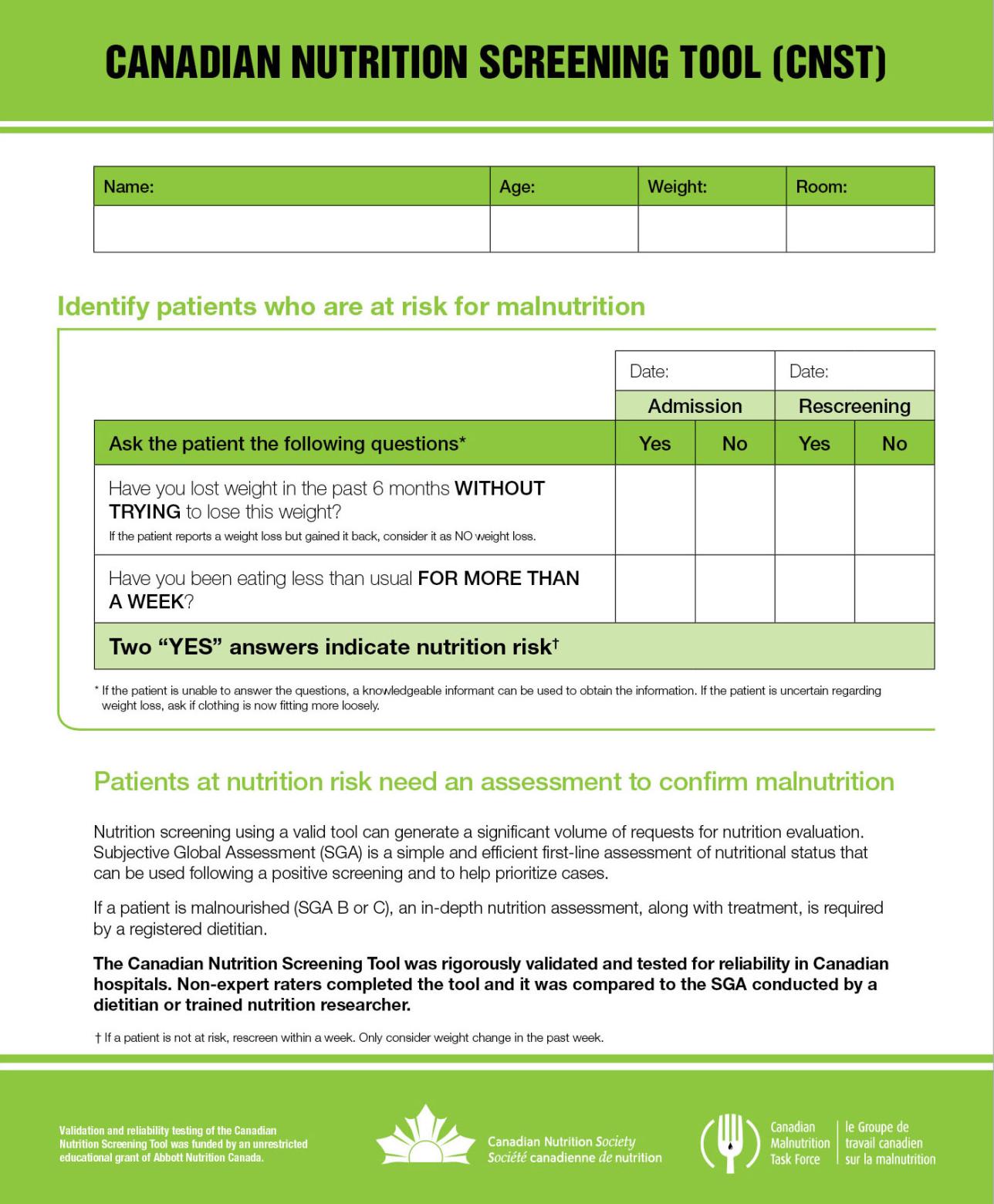
Screening Tools
The Canadian Nutrition Screening Tool (CNST) is a valid and reliable screening tool to identify those patients at risk of malnutrition in the adult acute care environment. (1)
Prehabilitation and Optimization Algorithm
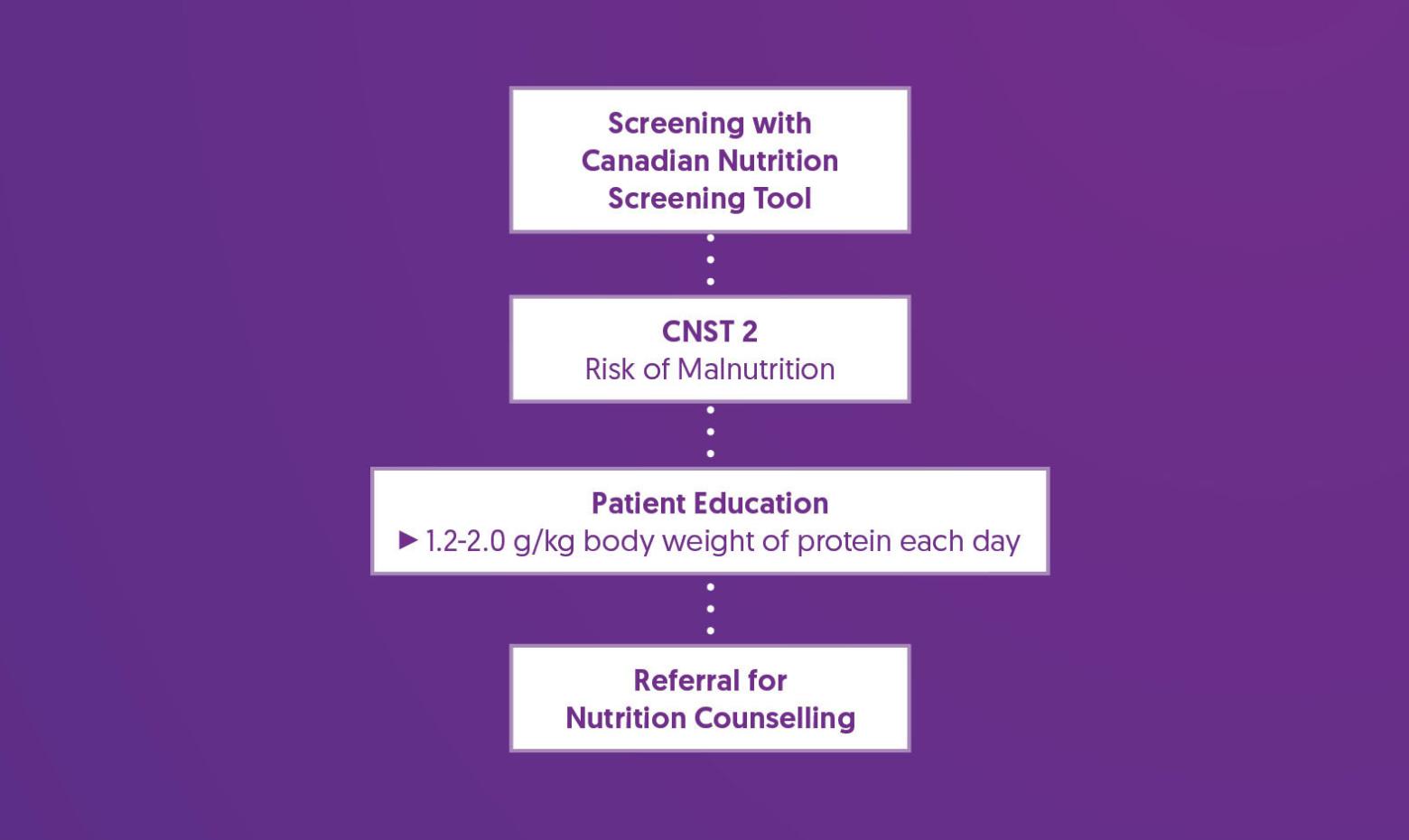
Prehabilitation and Optimization Recommendations
| Patient Education |
|
| Referral for Nutrition Counseling |
|
References
1. Laporte, M., Keller, H. H., Payette, H., Allard, J. P., Duerksen, D. R., Bernier, P., Jeejeebhoy, K., Gramlich, L., Davidson, B., Vesnaver, E., & Teterina, A. (2015). Validity and reliability of the new Canadian Nutrition Screening Tool in the 'real-world' hospital setting. European journal of clinical nutrition, 69(5), 558–564. https://doi.org/10.1038/ejcn.2014.270
2. Wong, H. M. K., Qi, D., Ma, B. H. M., Hou, P. Y., Kwong, C. K. W., Lee, A., & Prehab Study Group (2024). Multidisciplinary prehabilitation to improve frailty and functional capacity in high-risk elective surgical patients: a retrospective pilot study. Perioperative medicine (London, England), 13(1), 6. https://doi.org/10.1186/s13741-024-00359-x
3. Duerksen, D. R., Keller, H. H., Vesnaver, E., Laporte, M., Jeejeebhoy, K., Payette, H., Gramlich, L., Bernier, P., & Allard, J. P. (2016). Nurses' Perceptions Regarding the Prevalence, Detection, and Causes of Malnutrition in Canadian Hospitals: Results of a Canadian Malnutrition Task Force Survey. JPEN. Journal of parenteral and enteral nutrition, 40(1), 100–106. https://doi.org/10.1177/0148607114548227
4. Duerksen, D. R., Keller, H. H., Vesnaver, E., Allard, J. P., Bernier, P., Gramlich, L., Payette, H., Laporte, M., & Jeejeebhoy, K. (2015). Physicians' perceptions regarding the detection and management of malnutrition in Canadian hospitals: results of a Canadian Malnutrition Task Force survey. JPEN. Journal of parenteral and enteral nutrition, 39(4), 410–417. https://doi.org/10.1177/0148607114534731
5. Allard, J. P., Keller, H., Jeejeebhoy, K. N., Laporte, M., Duerksen, D. R., Gramlich, L., Payette, H., Bernier, P., Vesnaver, E., Davidson, B., Teterina, A., & Lou, W. (2016). Malnutrition at Hospital Admission-Contributors and Effect on Length of Stay: A Prospective Cohort Study From the Canadian Malnutrition Task Force. JPEN. Journal of parenteral and enteral nutrition, 40(4), 487–497. https://doi.org/10.1177/0148607114567902
6. Martínez-Ortega, A. J., Piñar-Gutiérrez, A., Serrano-Aguayo, P., González-Navarro, I., Remón-Ruíz, P. J., Pereira-Cunill, J. L., & García-Luna, P. P. (2022). Perioperative Nutritional Support: A Review of Current Literature. Nutrients, 14(8), 1601. https://doi.org/10.3390/nu14081601